Drugs designed to clear amyloid beta from the brain show no meaningful clinical benefit for Alzheimer's patients and increase the risk of brain swelling and bleeding, according to a major Cochrane review published May 4.
The analysis pooled results from 17 clinical trials involving 20,342 participants, all of whom had mild cognitive impairment or early-stage Alzheimer's dementia. These are the patient groups researchers have long believed offer the best window for treatment, on the theory that targeting amyloid early, before widespread neurological damage occurs, gives the drugs the best chance of working.
That theory has now taken a serious blow.
"Unfortunately, the evidence suggests that these drugs make no meaningful difference to patients," said lead author Francesco Nonino, a neurologist and epidemiologist at the IRCCS Institute of Neurological Sciences of Bologna, Italy. "There is now a convincing body of evidence converging on the conclusion that there is no clinically meaningful effect."
Nonino drew a pointed distinction between statistical and clinical significance. Several earlier trials found results that were statistically significant, meaning the effects were unlikely to be due to chance. But the actual measured improvements in memory and dementia severity fell well below the threshold considered meaningful in clinical practice. A drug can show a detectable effect on a trial's outcome measure while doing essentially nothing a patient or caregiver would notice.
The safety picture complicated matters further. Anti-amyloid drugs were linked to higher rates of brain swelling and microbleeds, a condition called ARIA, short for amyloid-related imaging abnormalities. In many cases these changes were only visible on MRI scans and produced no obvious symptoms. But long-term consequences remain unclear, partly because symptom reporting was inconsistent across the trials reviewed.
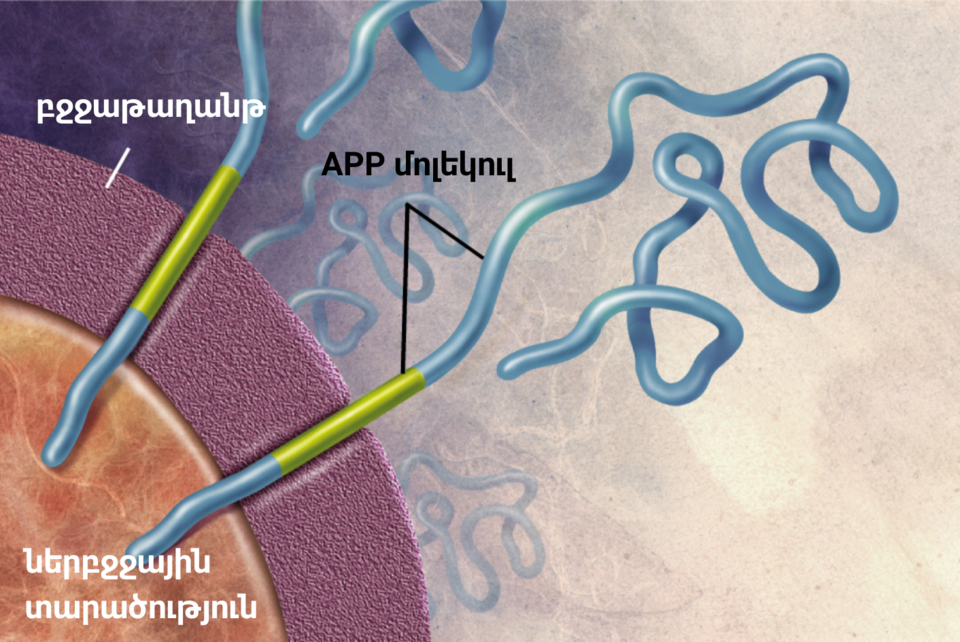
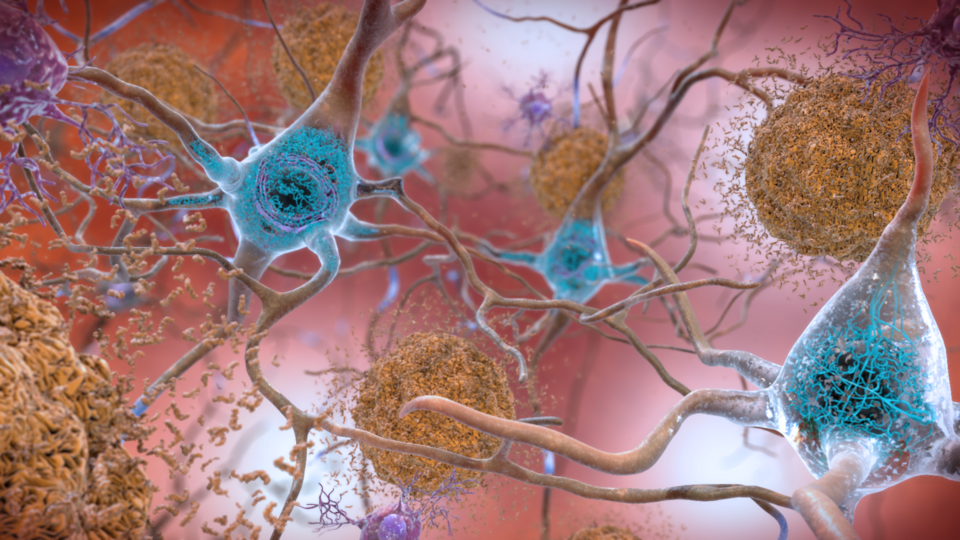
The amyloid hypothesis has dominated Alzheimer's research for decades. It holds that the buildup of amyloid beta plaques in the brain drives the disease, and that clearing those plaques should slow cognitive decline. Billions of dollars in research and drug development have followed that premise. Several anti-amyloid drugs have reached the market or late-stage trials, including lecanemab and donanemab, which received regulatory attention in recent years amid considerable controversy over their approval pathways and the clinical weight of their supporting data.
The Cochrane review does not name specific drugs but covers the class broadly. Its conclusions align with a growing body of critical literature suggesting the field may need to look beyond amyloid for answers. Researchers on the review said the evidence now argues against continuing to concentrate drug development resources on amyloid removal alone.
What comes next for Alzheimer's research is unsettled. Alternative targets, including tau proteins, neuroinflammation, and metabolic factors, have attracted increasing interest. But none has yet produced a drug with a convincing clinical track record. The Cochrane findings add pressure to that search without pointing clearly toward what should replace the amyloid approach.